
Fundamentals
Understanding how we can keep inventing medicines for patients and society and ensure biomedical innovations are affordable with insurance shouldn’t be complicated.
Read and watch our collected resources below to learn about the foundation for biomedical innovation, solutions to affordability, and the role of basic science, industry, investors, insurance, and government.
Health care policy is complicated and political, and it has a real-world impact on patients, their families, and society as a whole.
But we can improve it. First, though, we need to tease it apart systematically and judge it against some basic goals we can all agree on: e.g., we want today’s medicines to be affordable and we want scientists to keep working on inventing new, better ones.

NPLB’s 2+3 Improvements
We hope this resource page of “Fundamentals” will take you on an affordable innovation journey and make the case for two key improvements to our nation’s health care system:
-
If your insurance claims to cover something, it should be affordable to patients. We need a low out-of-pocket cap on what health insurance plans are allowed to charge their members for physician-prescribed treatments.
-
To get the maximal value from innovation intended by our long-standing patent system, we must be able to count on all drugs to go generic without undue delay after a patent-intended period of market-based pricing. So that means we need to fix the IRA’s 9-year pill penalty by changing when small molecules can be subjected to Medicare price setting (“Negotiation”) to be 13 years post launch, same as biologics. Ideally we would then also restore incentives for pediatric testing and other meaningful upgrades using six month extensions (to patents and/or when price setting kicks in).
When drugs go generic, it’s like society has paid off its mortgage (to the innovator, which you can think of as being like a home builder) and now enjoys the benefits of that drug at a public good at a low cost indefinitely. If a drug can’t go generic, then it can feel like the mortgage never ends, which means that the price of that drug really represents rent to society (making the innovator more of a Landlord). The patent system is designed to make sure that innovation is incentivized with temporary mortgages, not ongoing rent, and this ethos should be affirmed with policy that ensures that drugs become inexpensive when their intended mortgage period is up. If competition cannot achieve this end once a drug’s patent-protection expires, then price controls are warranted.
These two improvements represent the biotech social contract. These next three improvements are important, too, but, for the purposes of preserving affordable innovation, are less urgent than the first two. We break these up to ensure that the first two points really stand out.
-
To streamline patient access to medicines, Congress should mandate that prior authorizations be real-time, electronic, and as frictionless as possible to confirm a patient’s eligibility for a prescribed treatment. Today, insurers sometimes induce undue friction with gratuitously complex prior authorization forms and processes to wear down physicians and deter them from prescribing appropriate treatments; this is a feature of dishonest insurance since insurance plans can claim to cover a medicine but make it functionally inaccessible.
-
It is reasonable for America to incentivize companies to research and manufacture medicines in the US and countries with which it is geopolitically aligned to better insulate America’s biomedical supply chain from geopolitical instability.
-
America should ask its trade negotiators to encourage freeriding OECD countries (e.g., the UK, France, Canada, Australia, etc.) to pay more of their fair share for medicines to support the innovation they enjoy because of America’s willingness to pay (e.g., likely leveraging tariffs). This is analogous to calling for other countries to spend more on their militaries to contribute their fair share to global security. Such biopharmaceutical trade policy will also help address the resentment among Americans that they are unfairly paying far more than people in other developed countries, a source of outrage that, as with anger over high out-of-pocket costs, is sometimes misdirected at innovators, resulting in misguided calls for price controls.
Out-of-pocket costs are innovation kryptonite
American patients will be understandably angry as long as they are made to pay more than they can afford at the pharmacy for a properly prescribed medicine they need.
While it is appropriate for patients to be angry at their insurance plans for charging unjust out-of-pocket costs, some of that anger ends up misdirected at innovators to justify calls for price controls that will deter investment in continued innovation, as we are seeing today with the IRA’s small molecule penalty. Therefore out-of-pocket costs are the innovation kryptonite.
That’s why NPLB’s primary mission is to bring about out-of pocket caps. Capping these costs is the solution to making medicines affordable and protecting innovation.

Walking through the solution door
Reforming insurance with out-of-pocket caps and the other four recommendations are a solution set that lies beyond a doorway we hope you’ll walk through with us. But on the way to that solution door, we must pass by all the “but what about…?!” questions that represent side doors that divert us away from real solutions for affordability and innovation.
Some people will ask whether it’s true that NIH invents medicines so maybe companies shouldn’t be able to charge high prices. Some will wonder about patients having financial skin-in-the-game and whether copayments are necessary to prevent over-utilization of medicines. They will wonder why the US can’t pay less for medicines since companies sell them for less in Canada and other countries that do cost-effectiveness math to calculate what a medicine’s fair price should be.
The list of “what abouts” goes on and on. The resources on this page of Fundamentals and others in the Learn portion of the NPLB website answer these questions with data and analogies to make the case for affordable innovation for Americans (and the rest of the world).
We hope you find the arguments convincing (if not, let us know how we can improve them), so that you walk through the door with us to effective solutions that meaningfully improve affordability while preserving US innovation.
Investors, incentives, and public funding
Without the right incentives, most ideas will never leave the lab.
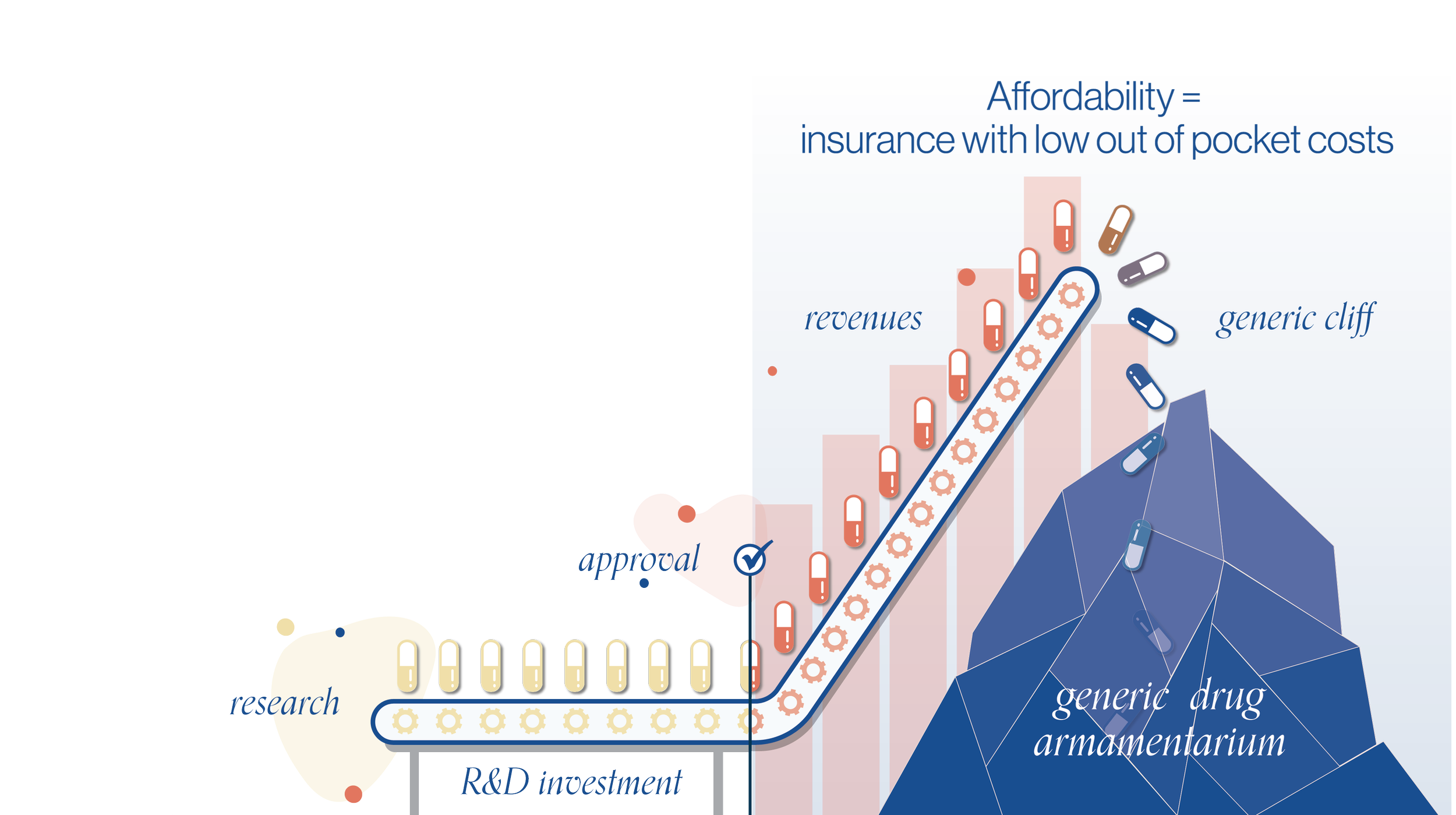
Publicly-funded basic science (e.g. NIH) provides the foundational insights that might lead to new medicines, but NIH scientists need industry’s innovators to actually create those medicines. Innovators rely on private investment (e.g. from individuals, pensions funds, venture capital, etc) to provide them with the necessary funding to test and develop their ideas into medicines. Investors expect a return to justify their investment, which means successfully developed medicines have to be profitable. Proper insurance (with low/no out of pocket costs) lets profitable medicines be affordable to patients. When those medicines go generic, all of society saves.
Doesn’t the NIH invent new medicines?

Inventing new medicines is a long climb
Who creates new medicines? It takes teams of innovators working with the support of private funding to reach risky new summits and provide patients with new cures.

The Investor’s Paradox
Drug development is costly. Who takes the risk and funds the hope of new medicines? Investors do. How do they know which ones will work? They often don't.
Why are drug prices so expensive to begin with? What’s the big deal about cutting the biggest selling drugs down to just being reasonably profitable?

How to Kill the Conversation that Makes Innovation Possible
Price controls harm innovation. Invention requires investment, and investors can only justify funding drug candidates they expect to eventually make money. Without the right incentives, investors will put their money in other industries, leaving patients with no hope for new cures.

How public funding, incentives, and private funding function together to enable all of us to get what we want: new medicines
Some think that the NIH can invent drugs alone. They can’t. Public funding provides the “base camp” knowledge necessary for discovery, but scientists—backed by private investors—must still dedicate years of research and billions of dollars to create new cures for patients.
Measuring the societal value of new medicines
Medicines do so much more than help the patients treated today.
When a sick person gets better, their family benefits, their caregivers are freed up to help others, and everyone’s joy and productivity is restored. And new drugs eventually become inexpensive generics, providing future generations the same benefit for little cost.
In assessing the value of innovative medicines to inform healthcare decision-making, backed by outdated math, some health economists, particularly outside the U.S., rely on outdated math which ignores these values. Unfortunately, that can result in patients being denied access to medicines that actually are worth paying for. When valuable new medicines are undervalued, we get fewer of them, and we all end up worse off.
Can’t we set prices based on the benefits of new medicines?

The Value of Medicines
Medicines do so much more than help the patient that's treated today. Considering a drug's societal value shows we may value them a lot more than we had thought.
Getting the math right when measuring the value of new medicines
Cost-effectiveness analysis (CEA) is commonly used to inform the assessment of value from new healthcare technologies. However, traditional CEA methods often fail to capture important components of social value for biopharmaceutical and other innovations. New research using updated & better math found that, when accounting for a drug’s societal value, drugs provide much more value than previously understood.
Why are drug prices cheaper in Europe and the rest of the world? Why should patients care if the U.S. adopts cost-effectiveness analysis?

Can the European scorpion hold its sting?
The U.S. market pays for much of the cost of inventing new medicines. European countries, hoping to reduce their spending, employ shortsighted and incomplete math to justify paying far less for medicines than they’re worth–and in some cases, denying patients access to new drugs. Not only is their math wrong, but underinvesting in new medicines today will mean paying more for hospital care in the future.

Battling the consequences of price controls at high altitude
In some U.S. states, Prescription Drug Affordability Review Boards (PDABs) are beginning to set the prices that insurance plans are able to pay for certain drugs at the state level. The criteria these new boards use is often vague and subjective, leaving patients without answers or access. Any attempt to determine a drug’s value should account for its societal benefits to all of us.

Aducanumab & the Alzheimer’s Moonshot: What Would It Be Worth to Keep Your Mind?
Alzheimer’s and diseases like it have horrible costs on individuals, caregivers, and their families. A treatment for Alzheimer’s would not only relieve suffering for the patient and their family, but it would increase the productivity of millions of Americans and lower direct and indirect costs associated with care. And, once the treatment becomes generic, it will permanently upgrade human health for much less.

For Two Years, Australia Failed People With Cystic Fibrosis; It Can’t Happen Again
Trikafta is a life-changing medication for people with Cystic Fibrosis. Unfortunately, governments around the world have withheld access for years in the name of being hawkish on drug pricing. This is a mistake. Besides the direct benefits to those suffering today with Trikafta, the drug benefits caregivers, communities, and future generations born with cystic fibrosis who will take Trikafta after it has become generic.
Insurance coverage–without high out-of-pocket costs
By buying insurance, we spread the cost of new medicines and innovation across everyone–not just sick people.
For insurance to really be insurance, it should fully cover the drugs your doctor prescribes when you’re sick–without high out-of-pocket costs. Otherwise, what’s the point of premiums?
Shouldn’t patients have to pay something for their prescribed medicines?

Affordability & Innovation: An Animation
Most of us pay for health insurance for many years while we’re healthy so that we can afford and access appropriate treatments when we get sick or injured. Yet many insurance plans still charge high out-of-pocket costs not everyone can afford for prescription drugs and other vital treatments – even those specifically authorized by their plan. This system needs reform.

What is Abbie Saving For?
High health plan copays are harming American families. Even with “insurance," one in four cannot afford them.

Healthcare Affordability & Innovation
Proper insurance should provide access to new cures with no out-of-pocket costs. New medicines ultimately benefit all of us. Society ought to pay for them together without burdening those who need them today with high out-of-pocket costs.
HCV: A case study on why innovation matters
It may seem like we have made all the progress we can in treating diseases. But that’s not the case. Everyday, scientists get closer to treating and curing diseases like Alzheimer’s and Cancer.
Medical progress over the last quarter century has reduced suffering and saved millions of lives. We need to preserve the incentives that make this progress possible. There’s so much more we can do.
Who cares about new innovation? Haven’t we made all the progress we can?

How We Cured Hepatitis C: 15 Years of Ingenuity, Investment, Risk, Failure, and Perseverance
This slide deck contains a powerful visual illustration of the biotech industry’s race to find a cure for Hepatitis C. Run through the slide deck quickly to appreciate the sheer level of hustle that won the world a cure, and then more slowly to appreciate every move in the role of proper incentives that made it possible for scientists to bring this cure from the lab to the pharmacy.
Expanding access and preserving the ecosystem
The right solutions are simple. We can protect the development of future cures without burdening today’s patients with high out-of-pocket costs.
Insurance should cover prescribed treatments without high out-of-pocket costs
Congress should strengthen existing laws and create new regulations that ensure that all medicines go generic without undue delay
We all should value the urgency to discover new medicines and protect the incentives for continued innovation.
I’m healthy. Why should I care about drug pricing policy and insurance reform?

Do more for patients, preserve innovation: Fix the Inflation Reduction Act
1000+ Investors, researchers, patients, & innovators urge critical fixes to Senate Rx Bill that can lower Medicare Rx deductibles, give the government greater power to set prices, and make sure biopharma research and development remains vigorous for both small molecule treatments and biologics.

Why fixing the IRA matters to all of us
Under the drug pricing provisions of the Inflation Reduction Act, small molecule treatments will face Medicare “negotiation” (price setting) that makes brand medicines functionally generic just 9 years after FDA approval. This policy will unwisely skew investment towards harder to manufacture biologics and away from small molecule treatments for diseases of aging. Without both kinds of medicines, we will all be worse off.

Investors and executives urge the Congressional Budget Office to adopt changes to its modeling
CBO’s ability to correctly model investor decision-making is vital to our country’s ability to establish policies that achieve lasting biomedical affordability and continued innovation. In support of CBO’s efforts to improve its model, this letter emphasizes a number of economic and financial first principles, notably that investment is incentivized by expected returns based on discounted profits, not revenue, and adjusted for expected dilution from financings.

Don’t F*** with the Density of Ice
Continued biomedical progress relies on an unappreciated foundation. Market-based pricing of new medicines for a patent-intended period of time combined with proper insurance with low out-of-pocket costs provide the necessary incentives for innovation and ensure broad access to new treatments.

Is the price right? Paying for value today to get more value tomorrow
Everyone should have access to timely, equitable, and cost-effective care covered by public funds, private insurance, or a combination of both. And we all benefit when new, more effective medicines are able to better manage disease, lowering total healthcare costs and increasing productivity. The expectation of adequate financial rewards motivates innovators and their investors to develop these new treatments. Discouraging the development of new medicines through price controls or by restricting coverage would ultimately cost society more and leave us all worse off.

US biosecurity starts at home, with insurance reform aimed at making innovation affordable
We can’t have true biosecurity without proper insurance reform. Americans won’t care who does or doesn’t make new medicines if they can’t afford them. Domestic price controls will only make America less competitive. Congress must pass out-of-pocket caps that promise affordability for all Americans.
Changing the conversation
When pricing drives the cultural conversation around new medicine, everyone loses.
To protect biomedical innovation and the incentives that drive it, we must do a better job creating fans of what we do and why we do it. The future of health depends on it.
If drugs are so valuable and insurance can make them affordable, how do we get Americans to stop being so angry at the drug industry's pricing practices every time it launches yet another novel medicine?

Eroding tolerance: A wonder drug shows us the drug industry’s fundamental failure to communicate.
Without proper communication, high prices erode the public’s support for the framework that makes innovation possible. Innovators, investors, and manufactures must do a better job conveying the value of new medicines to society and advocating for proper insurance reform that makes their medicines available with no out-of-pocket costs. Without the public’s support for continued innovation, we will all end up worse off—paying more for hospitals, surgeries, and nursing homes.

New DTC Marketing: Bringing our true customers along on our quest
For a long time, the drug industry took for granted that the value of the medicine they developed spoke for itself. That’s no longer true. Without a clear understanding of the work of drug manufacturers and the risks and costs of research and development, the public has lost its appetite for innovation. Manufacturers should inspire the public with advertising focused not on its medicines’ side effects but on the ongoing quest to permanently improve human health.